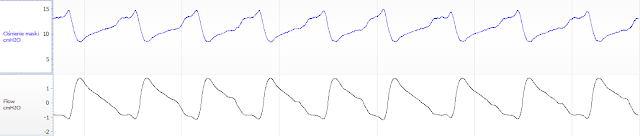
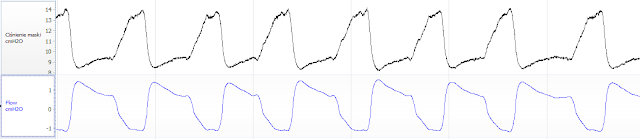
To be honest, I was very surprised – the inspiratory pause phase is practically nonexistent here… but there’s a suddenly a very extended expiratory phase! But maybe it’s a mistake, so let’s see how it looks in the VAUTO, also from ResMed:
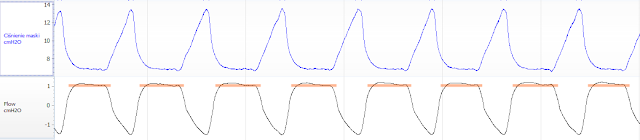
As you can see, the graph looks almost identical – so it seems to be a intentional characteristic of the device influencing the respiratory pattern we are dealing with at ResMed. The strong drop in the expiratory phase is, in my opinion, good (you can see that there is no resistance), the rounding of the graph in the last phase is a slight „pressure support” of the last phase of expiration.
Interestingly, despite the fact that it deviates from the natural breathing pattern, the device was more comfortable in perception than Philips. It probably lacks the option of maintaining pressure on inhalation (expiration is immediately initiated) and thus eliminates the pressure peak, which is perceived as slightly uncomfortable.
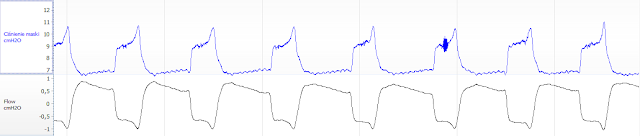
Let’s take a look at how it looks in other devices. First, Prisma from the German Lowenstein (similar to ResMed, however, you can see a slight „peak” on the exhalation, although the inspiratory pause is shorter. The extension of the inhalation phase is followed by the inhalation phase (slower inhalation, short pause and fast exhalation – again with a pressure peak at the phase change).
and also Blue from DeVilbiss (here the expiratory and inspiratory pause is beautifully outlined, but the device again has a problem with „letting go” and is therefore perceived as uncomfortable). The fluctuation in the graph may have been snoring, which has not been completely eliminated in this device.
They were all „branded” devices. But you’re probably wondering how Chinese devices are doing? There you go. Resvent first. Here we see only a small peak on the exhalation, clearly marked exhalation pause and shorter inhalation. It looks very good to me!
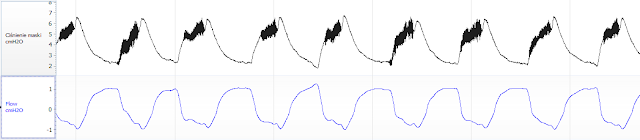
And last but not least, Apex (dark areas are nothing but very unstable pressure – the device „pulses” through the inefficient compressor all the time inhaling). Again, you can see a large peaked peak again at the exhalation and additionally a slow release of pressure (considerable internal resistance of the device).
What are the conclusions of all this for us?
First of all, it is clear how different CPAP devices are available on the market. Even Philips and ResMed, which in this study had very comparable clinical efficacy (measured by the reduction of AHI), differ diametrically in terms of how they affect the breath. You can stop laughing at me as I boast that I can often distinguish between CPAP by breath.
Secondly, I guess I don’t have to convince you that the expiratory relief actively influences the way you breathe with CPAP and thus significantly affects the comfort of the therapy. Apart from the infamous examples like APEX and DeVilbiss, most devices have good relief but their reception may be extremely different. You must be especially careful if you are disturbed by the pressure peaks at the end of the expiratory phase. It is better to try this CPAP before buying it.
Philips was the only one to actively lengthen the inhalation phase (inspiratory pause) so much, which could improve saturation at the expense of increasing CO2 levels (but this is not at all bad for a person with no CO2 retention problem because it stimulates the respiratory centre and prevents central apnea). However, this has been bought with a slight respiratory discomfort because there is a short increase in pressure in the last phase of inhalation. The same „trick” in the weaker technical DeVilbiss has been bought with a higher peak and an already serious comfort problem.
ResMed, in my opinion, does not try at all to reproduce the natural breathing curve and does not wait for an inspiratory pause, almost immediately letting go of pressure. I only guess that prolonging the expiratory pause is a direct consequence of this on a physiological level (otherwise there would be a significant increase in respiratory frequency). However, this resulted in the fact that – in my perception – the device was more comfortable. This does not mean, however, that it is due to the technological advantage – it is a more „technical trick” of the engineers. Looking at these graphs, we already know that introducing a „trigger” to the relief not at the end of the inhalation but at the moment when we want to make an exhalation, is simply very difficult and can increase the discomfort of the patient.
Are you curious how the elongation of both phases has affected the ventilation? So I was once again reaching for the results and it turned out that Philips did a little better with both ODI (desaturation index) 10.6:13.4 (Philips:ResMed) as well as I had a slightly better average saturation of 94.1:92:4 on it. However, already in AHI the competition was won by ResMed 2.16:1.30. This partly confirms my thesis that Philips’ approach slightly improves ventilation, but negatively affects the comfort of the therapy and has no clear impact on the final outcome of apnea therapy. I leave it up to you and your doctors to choose which device is better…
Finally, one more small comment. As I mentioned in the introduction, in this study the pressure was measured in the mask and not in the airways. So you don’t see one important and potentially dangerous condition. When breathing through CPAP, there is often a very bad phenomenon of negative airway pressure at the beginning of the inhalation phase. This phenomenon is intensified when the internal resistance of the device is high, which is the case with low quality CPAP (but also, for example, with clogged filters). Therefore, when buying CPAP always make a few quick, deeper inspirations and see if we do not feel resistance. If there is any resistance, let’s give up the purchase. The phenomenon may also occur to a lesser extent if the device is set to too low a pressure (the compressor works with reduced efficiency).